

Con infinito piacere, oggi apriamo le porte ad una delle colleghe più attive a livello internazionale nell’ambito della grande famiglia Alexander Discipline: la dottoressa Vjera Perkovic, direttamente da Rijeka, Croazia.
La Dottoressa Perkovic si è laureata in odontoiatria nel 2011, presso la Facoltà di Odontoiatria dell’Università di Zagabria ed ha conseguito la Specializzazione in Ortodonzia nel 2017, presso il Dipartimento di Ortodonzia dello stesso ateneo. Da gennaio ad aprile 2017 ha frequentato la Clinica Drs Alexanders, ad Arlington (Texas, USA), in qualità di visiting doctor.
Grazie al suo percorso formativo, alla passione per la Alexander Discipline ed alla sua esperienza nella clinica Alexander, Vjera ha partecipato alla realizzazione di un interessante lavoro, che tratta uno degli argomenti più cari alla nostra disciplina: la stabilità a lungo termine.
Non essendo necessario aggiungere altro, lasciamo la parola alla Dottoressa Perkovic!
Buona lettura e buona settimana a tutti.
V Perkovic, M Alexander, P Greer, E Kamenar, S Anic-Milosevic
Angle Orthod. 0000;00:000–000.
Long-term stability is something we as orthodontist specialist strive to achieve. There has always been a debate – is it possibile to achieve long-term stability after orthodontic treatment and how do we achieve it?
Dr. Wick Alexander, a founder of Alexander Discipline, recently passed away, but has left an enormus legacy to the orthodontic world. His „Room of Truth“ is basically a database of all patients treated at the office of Drs. Alexanders (Arlington, Texas, USA), where patients were treated by dr. Wick Alexander and dr. Moody Alexander following the principles of Alexander Discipline. Those principles are simple-treat patients in efficient way and achieve excellent results and long-term stable results.
THE AIM
The aim of this retrospective research was to investigate dental arch width changes 20 years after orthodontic treatment as well as what is long-term stability of patients 20 years after they were treated with Alexander Discipline orthodontic treatment.
THE WORK

Sample consisted of 103 patients from drs. Alexanders patient database, that were treated in the 1970s and 1980s by an experienced orthodontist – dr. Wick Alexander. Sample was collected from his private orthodontic clinic Drs Alexanders, Arlington, Texas, USA database (Picture 1).
Inclusion criteria were patients with
- initial Class I or Class II malocclusion treated with comprehensive orthodontic treatment with bonded fixed appliances in both arches,
- orthodontically treated with and without extraction of permanent premolars,
- full records before treatment, after treatment and post-retention period of at least five years.
Exclusion criteria were:
- missing permanent teeth (except third molars),
- class III patients and craniofacial anomalies,
- missing full records and
- circumferential supracrestal fiberotomy (CSF) performed.
Retention protocol lasted for three years with the following appliances: wraparound retainer in the upper arch and fixed retainer from canine to canine in the lower arch. Retention appliances were removed after three years and interproximal reduction (IPR) was performed in the lower intercanine segment in patients where this was not done during the orthodontic treatment.
Dental casts were obtained in three time periods: pretreatment (T1), post-treatment (T2), and long- term post retention of at least five years (T3). All dental casts were digitalized with an Ortho Insight 3D scanner (Motion View LLC, Hixon, USA) and converted to 3D dental casts (STL files).
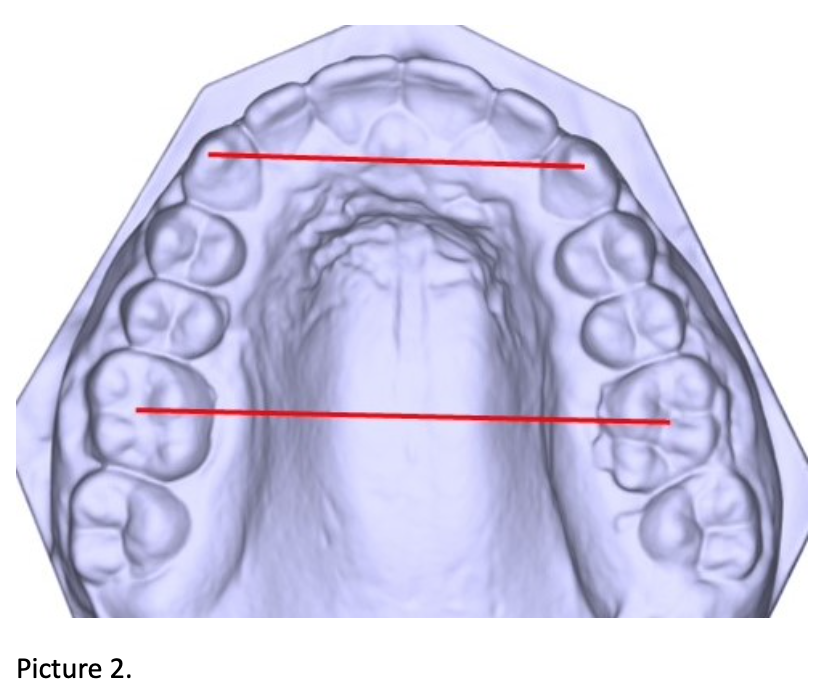
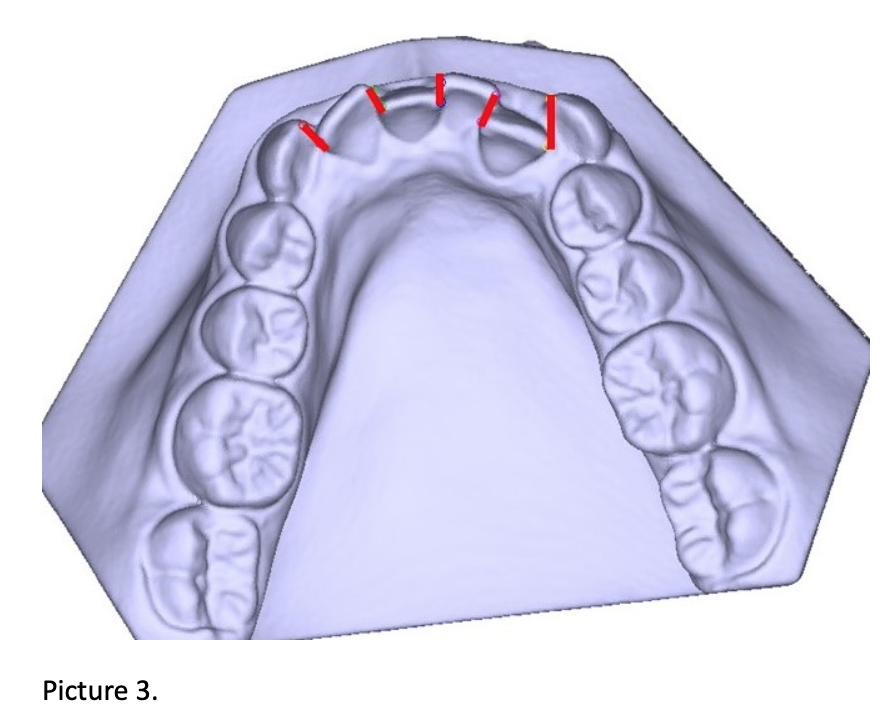
Linear measurements were evaluated in customized Matlab software, programmed for this research, for upper and lower arch in all three periods: Intercanine width (IC), Intermolar width (IM) and Little’s Irregularity Index (LII). (Picture 2 and Picture 3)
THE RESULTS
There were 73 female and 30 male patients. Class I was present in 74 patients and Class II in 29. Average post-retention time was 17.2 (±6.5) years with an average retention time of 3.4 (±1.17) years. Extraction was performed in 55 patients while 48 received non-extraction treatment. Bonferroni Post Hoc test showed that LII in the upper and lower arch in T1 was statistically significantly higher in the extraction group (P<0.001). Upper and lower arch LII in T3 was slightly higher in extraction cases but remained under 2.05mm. LII in T3 in the upper and lower arch showed a negative correlation with IM T3 in upper arch (Pearson,N=103, P=0.047), while IC in the upper and lower arch in T3 correlated with IM T3 in the upper and lower (N=103, P<0.001)
THE DISCUSSION
The present study showed minimal misalignment in the post-retention period with satisfactory alignment (LII under 3mm) in 95 (92.2%) cases in the upper arch, and 85 (82.5%) in lower arch. Overall, these results demonstrate excellent stability for such a long post-retention period. Although, a few studies have investigated long-term changes over 10 years post-treatment, these findings are in line with two other studies with similar post-retention time periods, but only with extraction cases. Other studies showed poor stability in the long term (more than 10 years). Even though long-term changes were investigated in previous literature, no predictors for long-term stability were established yet, though some clinical treatment guidelines for better stability were given.
The explanation for good stability of anterior alignment in both extraction and non-extraction cases in this study perhaps lies in the fact that good diagnostics and treatment decisions were made in the beginning. Many studies didn’t address this problem which resulted in inconsistent conclusions. We may assert now that when stability guidelines are not respected, instability is inevitable.
The orthodontist that had treated patients in this study, dr. Wick Alexander, previously developed a technique that has long-term stability as a treatment goal and incorporated his principles into a treating technique that promotes stability, such as keeping the teeth inside the basal bone, limiting proclination of lower incisors to 3 degrees, expansion of intercanine to a maximum of 1mm. This technique is what we know as Alexander Discipline. According to his philosophy, if teeth were placed in the appropriate positions during active treatment, the interproximal reduction was properly performed, and third molars were resolved, then the chance of the result remaining stable after retainer removal is excellent.
Another aspect that might contribute to stability in this study is interproximal reduction which was performed at the end of the retention period in lower intercanine segment. IPR was done only in cases where it was not done during the treatment, whether the treatment method was extraction or non-extraction. Contact points were modified into contact surfaces which is used as a stabilizing procedure.
Intercanine widths in non-extraction cases showed minimal changes (less than 0.5mm in both arches). In extraction cases, changes were greater, especially in the lower arch in long-term post-retention period (but remained less than 1mm).
Intermolar width showed to be associated with good stability in this research, but only in extraction cases in the upper arch. Greater change in intermolar width in extraction cases in the upper arch influenced stability in post-retention period.
Since good stability of dental arches was reported 17 years out of retention, findings of this study do not support research that are suggesting long-term use of fixed or removable retainers to maintain satisfactory alignment. In this study, retention protocol lasted for three years. This was considered important since patients were treated and retained throughout the critical growth ages when greatest irregularity changes happen.
When discussing long-term alignment, physiological changes in dental alignment should also be mentioned. There is a trend of arch constriction with age. This changes are sometimes called arch maturation. It can be difficult to distinguish relapse changes and normal occurrence due to aging. In untreated subjects, research has shown that in 10 years (from age 20 to 30) Little Irregularity Index in the lower arch increased only 1mm, while intercanine width decreased by 0.43mm. In this research, arch dimensions and alignment changes were minimal and similar to those reported in untreated subjects, especially in non-extraction cases.
This study has certain limitations. The sample was not randomly selected, but taken from a pool of previously treated patients. Additionally, treatment selection was not randomized but carefully selected. This will always be an issue, since this is not possible in orthodontics. There are specific rules where it is determined whether a case should be treated with or without extractions and we should accept that these groups should be distinguished. For the reasons above, results should be interpreted with caution.
THE CONCLUSIONS
Clinically relevant long-term stability in both arches was found in extraction and non-extraction cases. It is possible to achieve long-term stability after orthodontic treatment without retention appliances. Intermolar width and its change during orthodontic treatment was an influential factor on long-term stability in extraction cases.